


For today’s blog post, we offer our advice on the USDCI data element recommendations for patient data
For years, we’ve been talking about capturing the right data elements as part of the road to true health information exchange and interoperability.
The United States Core for Data Interoperability (USCDI) begins to articulate how that exchange will actually happen.
At the same time, USCDI continues to expand patient data models for master data, adding new elements for capture and exchange. Another round of additions is currently being debated. And while USCDI guidance can dictate what you need to capture, it doesn’t tell you how to do so.
Many healthcare organizations are beginning to realize that it’s not always realistic to standardize each source system, particularly with somewhat inflexible enterprise applications and EHRs. Instead, they are turning to a semantic, logical, centralized data model that has some flexibility to accommodate future changes.
Let’s look at what USCDI expansion means for you, what might come next, and how we can help you assess the impact on your own data — and begin benefiting from the new data elements.
What Is USCDI?
USCDI is a standardized set of health data classes and constituent data elements for nationwide, interoperable health information exchange. The ONC Cures Act Final Rule of 2020 included provisions to standardize health data classes to enable true nationwide, interoperable health information exchange.
To accomplish this, USCDI establishes a core set of data essential to supporting patient care. This replaces the previous Common Clinical Data Set in many use cases, such as:
- Transition of care documents
- Clinical information reconciliation and incorporation
- How patients view, download, and transmit their own health data
- Electronic reporting to public health agencies
- API access to data
What are the new requirements?
Version 1 was published in May 2021 and established a baseline for which data elements must be accessible through EHRs as part of health information exchange. The initial baseline included some elements that have not historically been captured in most EMPIs, such as race, ethnicity, and email. Enforcement of this data set in exchange is set for Dec 31, 2022.
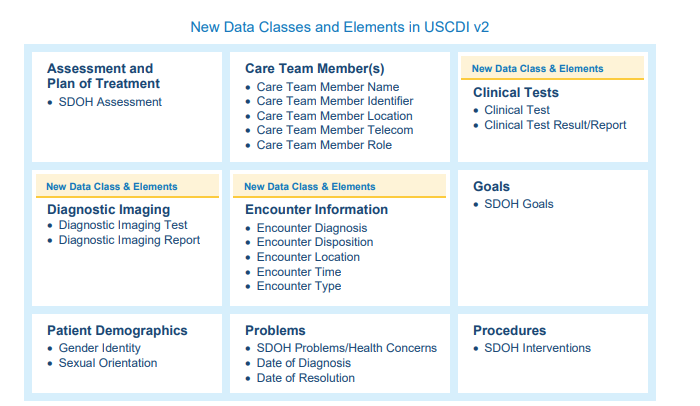
Version 2 was (published in July 2021) added several new elements pertaining to social determinants of health, sexual orientation, and gender identity among other test and result data for clinical and diagnostic tests, as well as a starting foundation for Social Determinants of Health (SDOH) assessments, problems, plans, goals and procedures..
Version 3 is currently under review and available for public feedback, with release scheduled for this summer. As proposed, Version 3 will add 20 data elements and two new data classes – health insurance information and health status.
New patient demographic elements will include:
- Date of death
- Tribal affiliation
- Related person’s name
- Related person’s relationship
- Occupation
- Occupation industry
Some of these data elements may already be under control and consistently captured and applied in your organization, but that day may only comply with data composition and code lists that are understood within your four walls. As interoperability and exchange mandates expand, a broader view must be applied to understand how to deliver upon semantic interoperability.
What USCDI means for healthcare organizations
USCDI dictates many elements that many healthcare organizations had previously omitted from EMPIs, such as Race, Ethnicity, and email address, either based on data availability or lack of standards for consistent data capture. Organizations that HAVE included these elements have not always done so in a consistent, shareable manner. And as more complex data elements are added, this challenge will continue to grow.
For organizations that have not yet fully standardized their data capture across all patient encounters, or who have had to deal with different data standards as a result of a merger or acquisition, USCDI offers some helpful guidance. R
Healthcare organizations should look carefully at what USCDI requires to begin aligning their own data capture practices. This has always been a challenge for organizations as they navigate mergers and acquisitions, as they must standardize their nomenclature between facilities. USCDI does help by defining what these elements should look like so you don’t need to start from scratch.
However, what do you do with all your existing data and systems? How can you standardize data across existing systems — while preparing for even more complex elements such as those for SDOH?
How IMT can help you prepare for alignment with USCDI
As we help clients plan for their USCDI alignment, we can help implement semantic, logical master data models to define these elements, enrichments and validations needed to transform and exchange legacy data with Health:iDM, with Semarchy xDM at the foundation.
It’s optimized for healthcare data, with a single platform for enterprise data modeling, matching, analytics, workflows, and custom reports so you can see how your data stacks up against USCDI requirements.
We can work with you to implement several elements for your USCDI strategy, including:
- A Business Glossary with versioning can help you manage data sets and code values as the standards evolve
- Data profiling for sources of new data elements before they are incorporated into your data hub, or released for sharing so you can confirm your data quality meets your organization’s standards
- Reference data management against SDOH code sets for data not typically stored centrally or to manage codeset version differences between different source and target systems
- A future-proof and agile platform to support evolving standards across current and future source systems and integration patterns
Start leveraging these new USCDI data elements now
USCDI shows promise at helping achieve the true interoperability we’ve long sought. That’s why we are encouraging our clients to begin voluntarily collecting this additional data ahead of the time when USCDI becomes a mandate.
Using these additional data elements can help you improve your matching and analytics, which can drive vital health equity and SDOH initiatives for your own community.
Talk to your stakeholders to discuss their big-picture goals so you can leverage your USCDI work to meet multiple goals. (And with Health:iDM, your stakeholders can leverage the same shared, integrated data framework for their own initiatives, without any additional coding.)
If you’re unsure about how to get started, get in touch. We have the knowledge to help, plus access to a growing variety of tools across our partner ecosystem.
Contact your IMT engagement lead or account manager or reach out to learn more. We can perform a data impact assessment to help you understand your existing data profiles and chart a roadmap for USCDI compliance and reaching your own initiatives.
